2026-05-29
[Real Case Review] Mini-Lifting, Corner Epicanthoplasty
Review of a 40s female patient's mini-lifting and corner epicanthoplasty at Weevers Plastic Surgery, addressing facial sagging and eye shape concerns.
![[Real Case Review] Mini-Lifting, Corner Epicanthoplasty](/uploads/uberps1/223970149272/a82955df14660a1b.png)
#CornerEpicanthoplasty #MiniLifting #Lifting #Epicanthoplasty #LateralCanthoplasty #MedialCanthoplasty #Weevers #WeeversPlasticSurgery #SeoSeungJo #ShimJeongHwan #Facelift #Cheeks #Jowls #NasolabialFolds #GangnamLifting #GangnamLateralCanthoplasty #GangnamEpicanthoplasty
Hello everyone~
your beauty universe! This is Weevers Plastic Surgery :)
Today, I'd like to review a case involving mini-lifting and corner epicanthoplasty.
Before Surgery


A female patient in her late 40s visited us concerned about sagging that extended from her anterior cheeks to her nasolabial folds and around her mouth.
She mentioned having undergone a mini-lifting at another clinic five years prior but didn't see significant results.
She was satisfied with the results of a thread lift performed at our clinic two years ago, which led to her returning.
This time, she came in considering a mini-lifting.
Her skin was inelastic and stretched easily, meaning a full facelift would actually be necessary to achieve a significant effect.
However, due to recovery time concerns, she wanted a less invasive procedure, so we planned a mini-lifting.


Additionally, she wanted to consult about corner epicanthoplasty because her outer eye corners felt 'stuffy'.
As she described, her eyes were large, but the outer corners felt blocked compared to the inner corners.
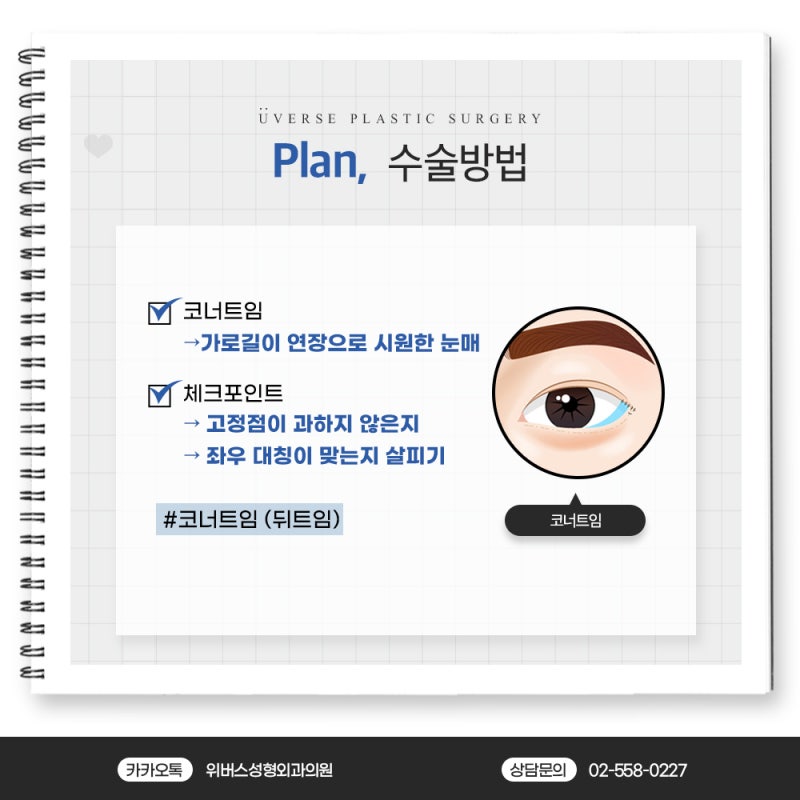
Therefore, we decided to extend the outer corners towards the earlobe to create a more refreshed eye shape.
Consultation and Surgical Process
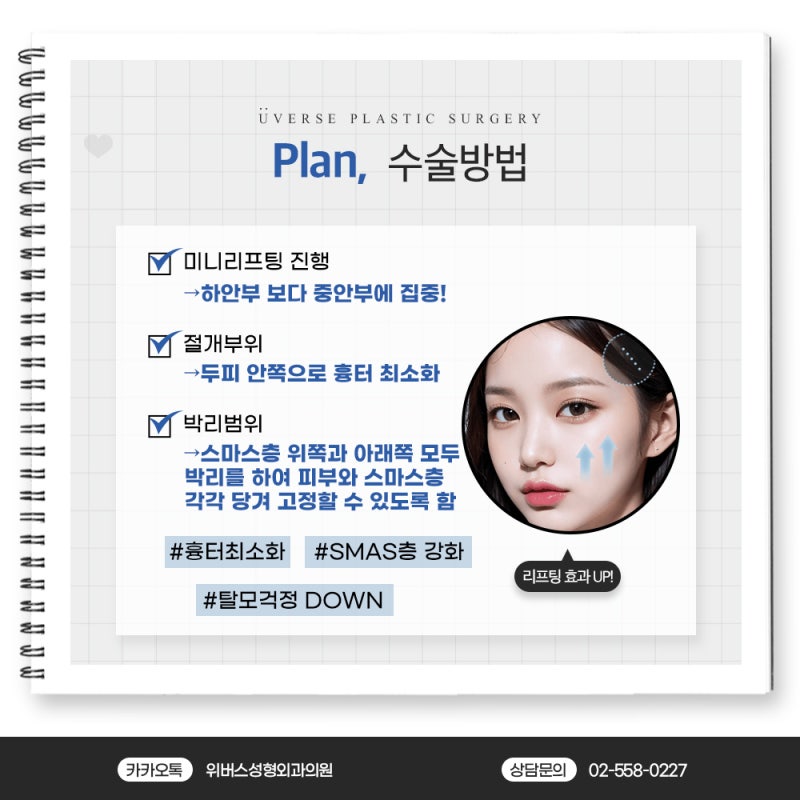
Given the extensive overall sagging, we decided to extend the incision for the mini-lifting further, up to the front of the tragus.
There was a scar from a previous surgery, and we designed the incision to include and remove this scar, ensuring the new scar would not be wider than the old one.
Extending the incision further allows for more lifting of the anterior cheeks and the area descending towards the mouth.
Following the usual method, we dissected above and below the SMAS layer, then pulled and sutured the SMAS layer.
At this point, excess tissue remains from the pull. If too much is left, the temple area might appear bulky.
Therefore, a portion of the SMAS layer is also excised to leave an appropriate volume.
Afterward, the remaining skin is trimmed with appropriate tension and sutured, followed by a compression dressing.
For corner epicanthoplasty, we dissected using the usual method and initially fixed it at appropriate anchor points.
During the surgery, the patient was asked to open her eyes to check if the current anchor points were not excessive and if the left and right sides were symmetrical.
If necessary, the existing fixation was released and re-fixed to find the optimal position suitable for the patient's eye condition.
Post-Surgical Progress
For mini-lifting, the patient visits the hospital the day after surgery to remove the dressing from the temple area and check for bleeding or fluid accumulation.
After this check, the wound can be managed by applying ointment without a compression dressing, allowing for normal daily activities.
Swelling primarily occurs in the temple area where the SMAS layer is pulled and sutured, but this area is mostly covered by hair.
In the patient's case, severe deep nasolabial folds were present, so Juvelook Volume was performed concurrently to alleviate them.
Since an extended incision mini-lifting was performed, even without direct manipulation of the jawline, the effect of pulling the SMAS and lifting the skin resulted in an improved jawline.
Looking at the photos one month later, the scalp scar became thinner than the original scar, and the scar in front of the tragus is not very noticeable. After about six months, once the scar matures, it becomes even less visible.
Want a quick consultation?


Frequently Asked Questions
Who is Mini-Lifting suitable for?
Mini-Lifting is suitable for individuals concerned about sagging in the cheeks, nasolabial folds, and mouth area. It is particularly an option for those who find a full facelift burdensome due to recovery time and wish to lightly improve sagging.
How far does the incision for Mini-Lifting surgery extend?
The Mini-Lifting incision usually extends to the front of the earlobe. This is to more effectively lift not only the cheeks but also the area descending towards the mouth, and if there are existing scars, they can be included in the design.
How is Corner Epicanthoplasty performed?
Corner Epicanthoplasty is performed by dissecting in the usual manner and fixing it to appropriate anchor points. During the surgery, the patient is asked to open their eyes to check if the anchor points are not excessive and if the left and right sides are symmetrical, and re-fixation is done if necessary to find the optimal eye shape.
When can I return to daily life after Mini-Lifting surgery?
The day after Mini-Lifting surgery, you will visit the hospital to remove the dressing from the temple area and check for bleeding. After that, you can manage it by just applying ointment without compression dressing, allowing you to return to daily life without significant disruption.
How noticeable are scars after Mini-Lifting?
Scars after Mini-Lifting gradually fade over time. Specifically, scalp scars become thinner than existing scars, and scars in front of the earlobe are not very noticeable; they become even less visible as they mature around 6 months.
Can other procedures be combined with Mini-Lifting?
Yes, it is possible. In this case, JUVÉLOOK Volume treatment was performed together to alleviate severe deep nasolabial folds. Additional necessary procedures can be combined according to individual concerns to enhance the overall improvement effect.